Spinal Fusion Surgery for Degenerative Disc Disease

A Fall. Six Months of Pain. His Spine Had Been Quietly Degenerating for Years.
At a Glance
| Patient | 55-year-old male |
| Complaint | Lower back pain for 6 months; difficulty walking and climbing stairs; tingling in left leg |
| Diagnosis | Severe disc degeneration at L4-L5 with degenerative changes at L2-L3 and L3-L4 |
| Procedure | Spinal fusion surgery at L4-L5 with stabilisation from L2 to L5 |
| Outcome | Lower back pain relieved; left leg tingling resolved; walking improved |
A 55-year-old man came in with a story many people will recognise. Six months earlier, he had a fall. After that, his lower back pain, which may have been building quietly for years, became impossible to ignore. Walking had become difficult. Climbing stairs had become a struggle. And a persistent tingling in his left leg had been with him ever since.
He had been managing it, hoping it would settle on its own. It did not.
For patients experiencing lumbar spondylosis or degenerative disc disease, symptoms like these are a sign that the spine needs proper evaluation, not just pain management.

Figure: X-ray on arrival showing degenerative changes across the lumbar spine
What Did the Scans Show?
Imaging confirmed that multiple discs across the lower spine had degenerated, and the damage at L4-L5 was severe enough to require surgical intervention.
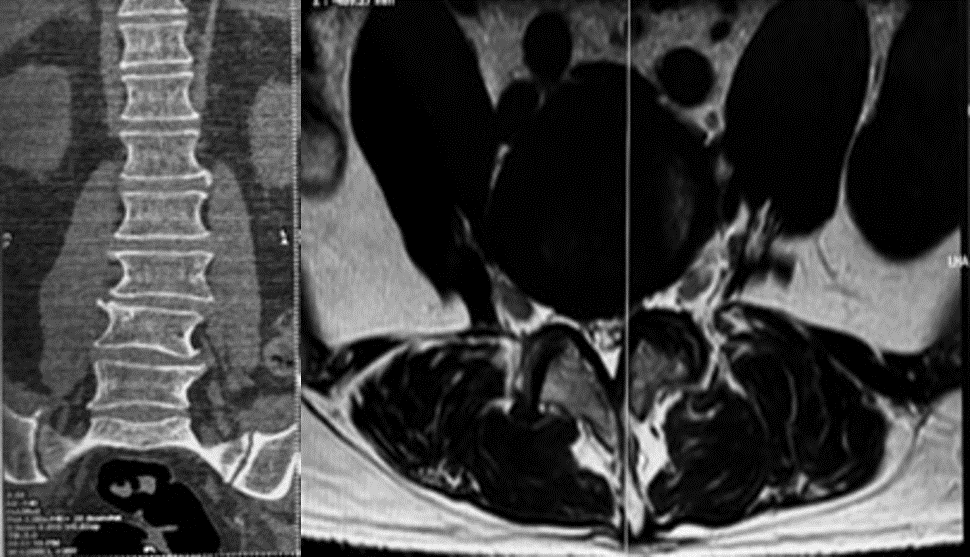
Figure: MRI showing severe disc degeneration at L4-L5 and degenerative changes at L2-L3 and L3-L4
The MRI showed degeneration across multiple levels of the lumbar spine. The discs, the cushioning pads that sit between each vertebra, had lost their normal height, hydration, and structure at L2-L3, L3-L4, and most significantly at L4-L5. When a disc degenerates severely, it can no longer absorb load or maintain the correct space between vertebrae.
The result is pressure on the nerves running through that region, which explained the tingling travelling down his left leg.
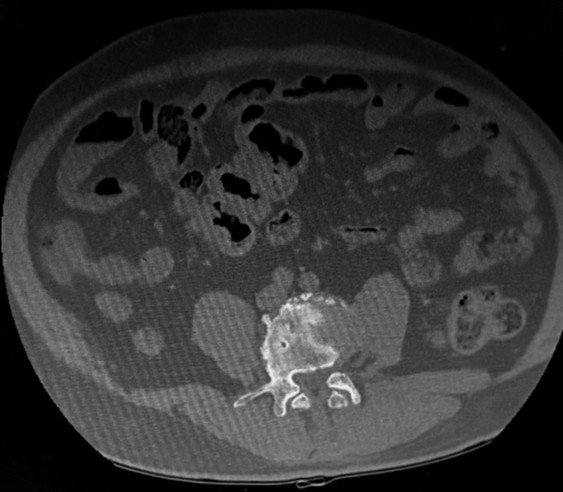
Figure: CT scan showing a transitional vertebra at the lumbosacral junction and Schmorl’s node at L5
The CT scan added two clinically important details.
- First, a lumbosacral transitional vertebra, a common anatomical variation where the boundary between the lumbar spine and the sacrum is slightly different from the norm, was present. This variation alters the way load is distributed across the lower spine and can contribute to faster degeneration over time.
- Second, a Schmorl’s node was seen at L5, a small indentation where disc material had pushed into the vertebral body, a sign of long-standing degenerative stress on the spine.
Reach Out for Expert Care
The Challenge
The damage was not limited to one level. Multiple discs were involved, and the surgical plan had to address all of them.
At L4-L5, the degeneration was severe enough that the disc could no longer support the spine. This level needed to be fused, but the levels above, L2-L3 and L3-L4, had also degenerated significantly, meaning they needed to be stabilised as well to prevent the problem from worsening after surgery.
The additional finding of a transitional vertebra meant the anatomy of this spine was unusual. Accurate level identification and careful pre-surgical planning were essential before any instrumentation was placed.
Procedure: What Was Done?
Spinal fusion surgery at L4-L5 with spinal fixation from L2 to L5 was performed, treating the most damaged level while stabilising the full degenerative segment.
At L4-L5, a procedure called Transforaminal Lumbar Interbody Fusion (TLIF) was performed.
In simple terms: the damaged disc was removed, and a small cage packed with bone graft material was placed in the disc space.
This cage maintains the correct height between the two vertebrae and allows the bones to gradually fuse into one stable unit over time, eliminating the painful movement at that degenerated level and relieving the pressure on the nerve.
Pedicle screws and rods were then placed from L2 to L5, anchoring the fusion and stabilising the entire affected segment of the lumbar spine.

Figure: Post-operative X-ray confirming spinal fusion implants correctly positioned from L2 to L5
The post-operative X-ray confirmed the implants were correctly positioned across all treated levels.
Outcome
Following lumbar spine surgery, the patient experienced significant relief from his lower back pain. The tingling in his left leg, caused by the compressed nerve at L4-L5, resolved after decompression and fusion. His ability to walk and manage stairs improved meaningfully.
Why Does This Case Matter?
Degenerative disc disease is one of the most common, and most under-investigated, causes of lower back pain in adults over 50. When it reaches the point of affecting daily movement and causing nerve symptoms, it needs more than pain relief.
Many patients with lumbar spondylosis or disc degeneration spend months managing symptoms conservatively, which is appropriate in the early stages. But when walking becomes difficult, when leg tingling or numbness appears, and when quality of life is steadily eroding, a surgical evaluation becomes a serious and worthwhile consideration.
This case also highlights something important: a fall does not always cause spinal degeneration. In many patients, the discs have been wearing down silently for years, and a fall simply brings the underlying problem to the surface. Treating the fall alone misses the bigger picture.
If you have been managing lower back pain with leg tingling or weakness, and it is getting worse rather than better, a proper spinal evaluation is the right next step.
Learn more about Spinal Fusion Surgery in Delhi, Spinal Fixation Surgery, Minimally Invasive Spine Surgery, and Lumbar Spondylosis, or book a consultation for a thorough evaluation.
This case study is published for educational and awareness purposes only. It does not constitute medical advice.
