Spinal Fusion Surgery for Disc Prolapse and Spinal Instability
She Had Been Managing the Pain for Months. Then One Morning, She Could Barely Move.
At a Glance
| Patient | 72-year-old female |
| Complaint | Severe lower back pain and right thigh pain for 2–3 months; sudden severe worsening over 2 days |
| Diagnosis | L1-L2 disc prolapse with spinal instability; degenerative changes across multiple levels |
| Procedure | Spinal fusion at L1-L2 with disc removal; stabilisation from D12 to L3 |
| Outcome | Significant pain relief; mobility restored |
A 72-year-old woman had been living with severe lower back pain and pain radiating into her right thigh for two to three months. It had been difficult, but manageable. Then, without warning, the pain became dramatically worse over just two days. What had been uncomfortable became debilitating.
She came in urgently. And the scans explained exactly why.

X-ray on arrival showing partial straightening of the lumbar spine and sacralisation of L5 – both signs of long-standing degenerative change.
Reach Out for Expert Care
What Did The Scan Show?
Imaging revealed a prolapsed disc at L1-L2 compressing the nerve, on top of widespread degenerative changes that had been building silently for years.

MRI showing disc prolapse at L1-L2 with nerve compression, ligamentum flavum thickening, and degenerative changes across multiple levels.
The MRI showed significant degenerative changes across multiple levels of the spine, discs that had dried out, lost their normal height and cushioning ability, and bulged outward at several levels.
The ligamentum flavum, a protective ligament running along the back of the spinal canal, had thickened at L4-L5, further narrowing the space available for the nerves. Facet joint arthropathy, a form of spinal joint wear, was also present at L4-L5.
The primary problem was clear: a disc prolapse at L1-L2; the disc had pushed out of its normal position and was pressing directly on the nerve responsible for sensation in the right thigh. This explained both her thigh pain and the sudden worsening that had brought her in.

CT scan showing Schmorl’s nodes and mild anterior wedge compression of D12, signs of chronic degenerative stress on the spine.
The CT scan added further detail: Schmorl’s nodes were visible, indicating long-standing degenerative stress where disc material had pushed into the vertebral bodies over time. A mild anterior wedge compression of the D12 vertebra was also noted, a sign that this spine had been under significant degenerative load for years before the acute episode.
The Challenge
This was not simply a disc prolapse in an otherwise healthy spine. It was an acute crisis on top of years of accumulated spinal degeneration, in a 72-year-old patient.
The disc prolapse at L1-L2 had caused the sudden severe pain, but the spine around it was also unstable, with degeneration at multiple levels, joint wear, ligament thickening, and vertebral compression all contributing to an already compromised structure.
Simply removing the disc would not be enough. The spine needed to be stabilised above and below the affected level to prevent further collapse, relieve pressure on the nerves, and provide this 72-year-old patient with a durable, long-term solution.
TLIF Procedure: What Was Done?
Spinal fusion surgery was performed at L1-L2 with disc removal, combined with stabilisation from D12 to L3.
At L1-L2, a TLIF (Transforaminal Lumbar Interbody Fusion) procedure was performed. In simple terms: the prolapsed disc that had been pressing on the nerve was carefully removed. A small cage packed with bone graft material was placed in the disc space to restore the correct height between the vertebrae and allow them to fuse into one stable unit over time. This directly relieved the pressure causing the back and thigh pain.
Pedicle screws and rods were then placed from D12 to L3, the vertebrae above and below the fused level, locking the spine in correct alignment and stabilising the full affected segment.

Post-operative X-ray confirming screw and rod fixation from D12 to L3, with implants correctly positioned.
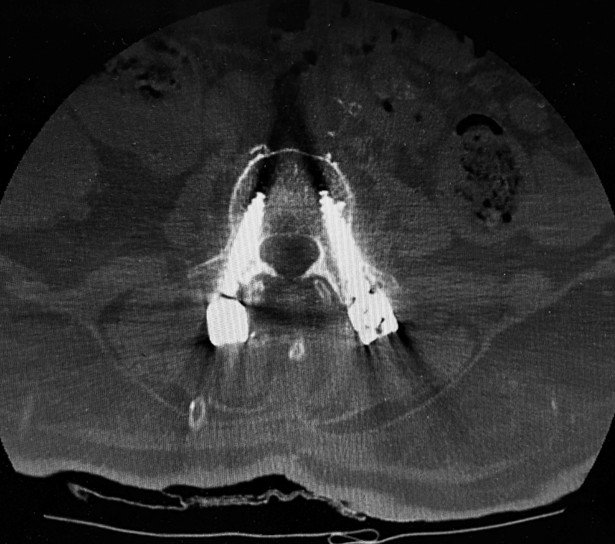
Post-operative CT scan confirming that the pedicle screws and rods are correctly placed from D12 to L3.
Both the post-operative X-ray and CT scan confirmed the implants were correctly positioned and the stabilisation construct was well placed across all treated levels.
Outcome
Following lumbar spine surgery, the patient experienced significant relief from both her lower back pain and the radiating pain in her right thigh. Mobility was restored, and she was able to move with far greater comfort than when she had arrived.
For a 72-year-old woman who had come in barely able to move, this was a meaningful and life-changing recovery.
Why Does This Case Matter?
Sudden severe worsening of back pain in an elderly person is never something to wait out at home. It is a signal to seek urgent evaluation.
This case illustrates two important points:
- First, years of gradual spinal degeneration can remain manageable until one additional event, in this case an acute disc prolapse, tips the balance and causes a sudden crisis.
- Second, treating that crisis effectively in an elderly patient requires understanding the full picture of the spine, not just the acute problem, but the underlying instability that made it possible.
Back pain that travels into the thigh or leg, known as radiculopathy, is a sign that a nerve is being compressed somewhere in the spine. In older adults, this symptom alongside sudden worsening of pain requires prompt imaging and specialist evaluation.
Delaying treatment in cases like this risks further nerve damage and a harder recovery. Early intervention, even in elderly patients, can restore function and quality of life meaningfully.
Learn more about Slip Disc Treatment in Delhi, Spinal Fixation Surgery, Lumbar Spondylosis, and Minimally Invasive Spine Surgery or book a consultation for a thorough spinal evaluation.
This case study is published for educational and awareness purposes only. It does not constitute medical advice. Seek immediate care for sudden or severe spinal symptoms.
