Minimally Invasive Spine Fixation with Tumour Biopsy
Reach Out for Expert Care
She Came in Unable to Walk. The Fracture Was Just the Beginning.
At a Glance
| Patient | 73-year-old female |
| Complaint | Severe lower back pain; difficulty standing and walking |
| Diagnosis | D11 vertebral fracture caused by multiple myeloma |
| Procedure | Minimally invasive pedicle screw and rod fixation (D9-D12, L1) with biopsy at D11 |
| Outcome | Pain relief achieved; mobilised at discharge; referred for radiotherapy |
A 73-year-old woman came in with severe lower back pain that had been making it increasingly difficult to stand up or walk. She was frail, elderly, and in significant discomfort.
Initial investigations raised a concern beyond a simple fracture: multiple myeloma, a type of blood cancer that can silently weaken bones from within, was suspected as the underlying cause.
The fracture needed to be stabilised, but first, the cause needed to be confirmed.

Pre-operative X-ray: X-ray on arrival showing diffuse bone weakness and changes at the D11 vertebral level.
What did the scans show?
Imaging revealed a fractured vertebra caused by a destructive lesion, not by a fall or injury, but from within the bone itself.
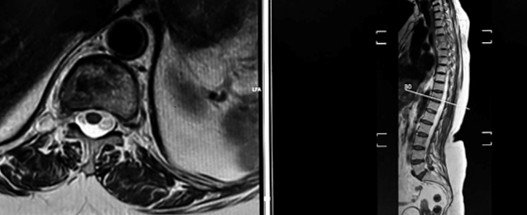
Pre-operative MRI: MRI showing the D11 lesion with vertebral involvement and additional disc changes at the lumbar spine.
The MRI identified a significant lesion at the D11 vertebra, the eleventh thoracic vertebra in the mid-back region, along with mild disc bulges at the lower back levels. The D11 lesion was the primary concern: it had weakened the vertebra to the point of fracture.

Pre-operative CT Scan: CT scan confirming pathological fracture of D11 due to a lytic lesion, bone being destroyed from within.
The CT scan confirmed what the MRI had suggested: a pathological fracture of D11. The word “pathological” is important here; it means the fracture did not happen because of a fall or trauma. It happened because the bone had been destroyed from within by a lytic lesion, a characteristic feature of multiple myeloma where cancer cells eat away at bone tissue, leaving it too weak to hold its structure.
The X-ray findings reinforced this, showing diffuse osteopenia (widespread bone thinning), prominent endplates, and marginal osteophyte formation across the spine, all consistent with the systemic bone involvement seen in myeloma.
The Challenge
This was not a straightforward spinal fracture. It was a fracture caused by cancer, and treating it required addressing both problems simultaneously.
In a 73-year-old patient with confirmed myeloma and a fractured vertebra, the surgical goal was twofold: stabilise the spine to relieve pain and restore the ability to move, and obtain a tissue biopsy from the D11 lesion to confirm the diagnosis and guide further oncological treatment.
Operating on an elderly patient with systemic bone disease requires careful planning. The bones are fragile, the surgical risk is higher, and the implants must be placed with precision in bone that may not hold as well as in a younger, healthier spine.
Procedure: What Was Done?
Dr. Vikas Gupta performed a minimally invasive posterior spinal fixation with biopsy, stabilising the fractured vertebra while simultaneously obtaining tissue for diagnosis.
Pedicle screws were placed at D9, D10, D12, and L1, the vertebrae above and below the fractured D11, and connected with rods to lock the spine in stable alignment.
On the left side, a screw was also placed at D11 itself to complete the construct. This minimally invasive approach was chosen specifically to reduce surgical trauma in an elderly, frail patient, with smaller incisions, less blood loss, and a faster recovery than open surgery would allow.
At the same time, a biopsy of the D11 lesion was taken, and a tissue sample was sent for laboratory analysis to confirm the diagnosis. The biopsy confirmed multiple myeloma.
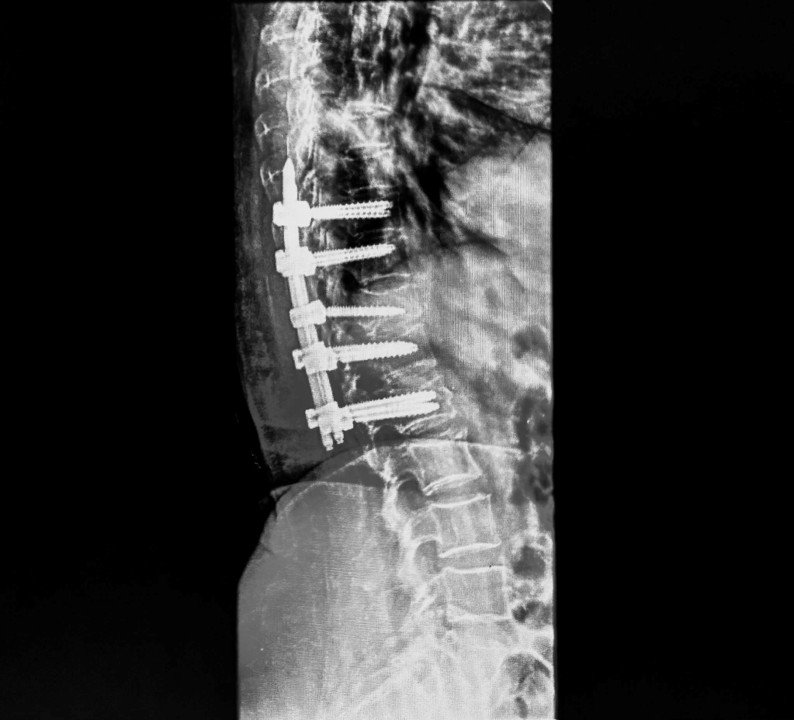
Post-operative X-ray: Post-operative X-ray confirming pedicle screws in the correct position across D9-D12 and L1, with D11 fracture stabilised.
Outcome
Following surgery, the patient experienced meaningful pain relief. She was able to stand and begin mobilising, a significant improvement from the difficulty walking that had brought her in. She was discharged on day 17 with physiotherapy and mobilisation guidance.
With the diagnosis of multiple myeloma now confirmed through the biopsy, she was referred for radiotherapy, the next step in managing the underlying cancer that had caused the fracture in the first place. Surgery had done what it needed to: relieve the pain, stabilise the spine, and give her oncology team the confirmed diagnosis they needed to proceed.
Why Does This Case Matter?
Not every spinal fracture is caused by a fall. In older adults, a fracture that appears without any injury is a warning sign that must be investigated.
This case is an important reminder that back pain in elderly patients, particularly when it is severe, progressive, and unexplained by any obvious cause, warrants thorough investigation. A fracture that happens on its own, without trauma, is called a pathological fracture. It means something else is going on inside the bone. In this case, it was multiple myeloma.
The surgical approach here served two critical purposes: it gave the patient her mobility and pain relief back, and it provided the tissue diagnosis that made further cancer treatment possible. Without the biopsy, the myeloma may have gone unconfirmed and untreated for longer.
For families of elderly patients: if a parent or grandparent develops sudden or worsening back pain, especially with no clear injury, do not assume it is simply age or arthritis. A proper evaluation with imaging can find conditions that are serious but treatable when caught in time.
Concerned about unexplained back pain or a spinal fracture in an elderly family member? Book a consultation with Dr. Vikas Gupta for a thorough evaluation.
This case study is published for educational and awareness purposes only. It does not constitute medical advice.
