Normal Pressure Hydrocephalus (NPH): Is It Aging Or Something Treatable?

When an elderly parent starts shuffling instead of walking normally, forgetting things, and losing bladder control, most families assume it’s just age. Sometimes, though, it isn’t.
Normal Pressure Hydrocephalus (NPH) is a brain condition in which excess cerebrospinal fluid (CSF) builds up, enlarging the brain’s ventricles and pressing on structures that control movement, memory, and bladder function. Despite this buildup, the fluid pressure often reads as normal on a spinal tap, which is how it gets its confusing name.
What makes NPH genuinely different from Alzheimer’s or Parkinson’s? It can be treated. In many patients, the right surgery reverses the symptoms significantly, something that isn’t possible with most other causes of dementia.
Reach Out for Expert Care
The Classic Triad: Three Symptoms That Point to NPH
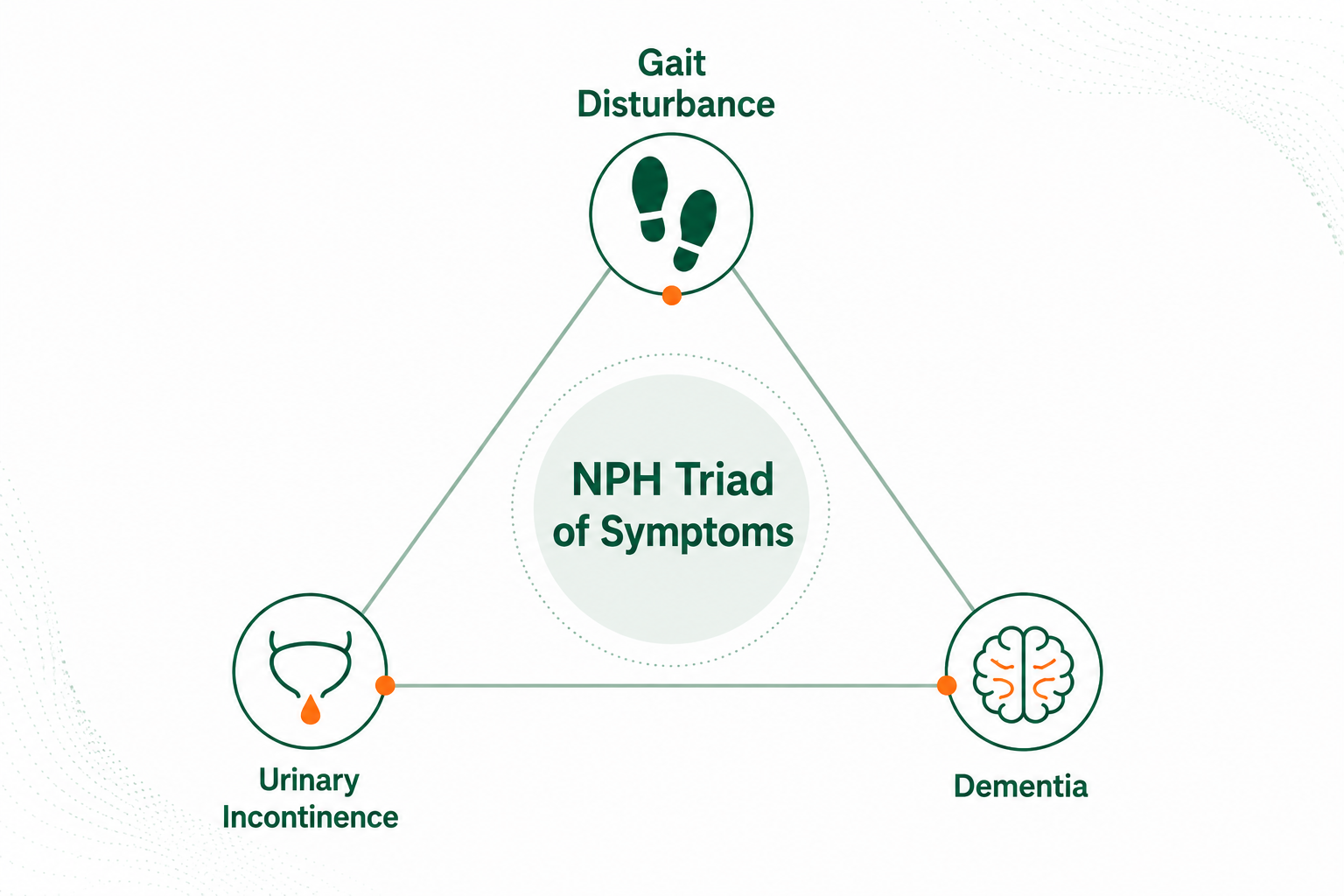
Doctors look for three symptoms appearing together:
1. Gait Disturbance – “Magnetic Gait”
Gait disturbance is usually the first and most prominent symptom of NPH. The person walks with slow, shuffling, wide-based steps – as if their feet are magnetically attached to the floor. This is called “magnetic gait.” They may have difficulty starting to walk, turning around, climbing stairs, and are prone to frequent falls.
Unlike Parkinson’s disease (where the stance is narrow), NPH gait is wide-based with outward rotation of feet. This symptom also has the best chance of improvement following treatment.
2. Urinary Incontinence
Bladder control problems in NPH are not related to any urological disease. They arise because the pressure on brain pathways controlling the bladder impairs the ability to sense the urge to urinate in time. Patients often experience increased urgency and frequency. In many cases, the slow gait itself prevents the person from reaching the toilet in time.
It is important to note that incontinence alone is not sufficient for an NPH diagnosis – it must be assessed alongside the other two symptoms.
3. Cognitive Impairment (Dementia-Like Symptoms)
NPH causes a slowing of mental processes rather than the memory destruction seen in Alzheimer’s disease. Patients show decreased attention span, mental slowing, reduced short-term memory, and poor executive function. Behavioural changes such as apathy, confusion, and disorientation may also be observed.
SInce these features overlap with Alzheimer’s and Parkinson’s diseases, many NPH patients are incorrectly diagnosed. The key difference is that NPH-related cognitive symptoms can significantly improve after shunt treatment, while Alzheimer’s cannot.
What Causes Normal Pressure Hydrocephalus?
NPH can be either idiopathic (no identifiable cause) or secondary (caused by another condition). Idiopathic NPH is the more common form and predominantly affects older adults.
Secondary NPH may develop following:
- A prior brain haemorrhage or subarachnoid haemorrhage
- Head injury or spinal injury
- Meningitis or brain infections
- Prior brain surgery
In secondary cases, disruption to the normal flow and absorption of CSF leads to gradual fluid accumulation. In idiopathic cases, the exact trigger remains unclear, though age-related changes in CSF dynamics are believed to play a role.
How Is NPH Different from Alzheimer’s and Parkinson’s Disease?
Many families bring their loved ones for evaluation after symptoms are misattributed to aging or other neurological conditions. The table below reflects how NPH symptoms compare:
| Symptom | NPH | Alzheimer’s | Parkinson’s |
| Gait Disturbance | First symptom (wide-based shuffle) | Partial / late | May present (narrow stance) |
| Memory / Thinking Problems | Mental slowing | Prominent | Partial |
| Urinary Incontinence | Present | Partial | Partial |
| Tremor of Limbs | Not present | Not Present | Present |
| Bradykinesia | Not present | Not present | Present |
This differentiation matters enormously because NPH is treatable and potentially reversible, making early and correct diagnosis life-changing.
If an elderly family member has been told they have dementia but also walks unusually slowly, it’s worth getting a second opinion. Alzheimer’s care in Delhi →
How is NPH Diagnosed?
Accurate diagnosis of NPH requires a combination of clinical evaluation and imaging, following a structured diagnostic pathway.
Step 1 – Clinical Examination: The doctor assesses whether any element of the classic triad is present. If no triad element is found, other conditions are evaluated.
Step 2 – Neuroimaging (CT / MRI of the Brain): If triad symptoms are present, brain imaging is performed. NPH is confirmed radiographically by:
- Moderate to severe ventricular enlargement (ventriculomegaly) disproportionate to cerebral atrophy
- Evans Index of greater than 0.3 (the ratio of frontal horn width to inner skull diameter)
- Ballooned frontal horns, enlarged temporal horns, callosal angle greater than 40 degrees
Step 3 – Evaluate Surgical Candidacy: Once NPH is confirmed radiographically, the patient is evaluated for suitability for shunt surgery. This includes:
- LP (Lumbar Puncture) CSF Tap Test: A large-volume CSF withdrawal (30-50 ml) is performed. If gait, cognition, or continence improves significantly after the tap, it predicts a good response to shunt surgery.
- In cases where the tap test is inconclusive, External Lumbar Drainage (ELD) over 3 days provides further evidence.
Step 4 – Confirm and Proceed with Treatment: If surgical candidacy is confirmed, the neurosurgical team proceeds with shunt placement.
Treatment for Normal Pressure Hydrocephalus in Delhi
The primary treatment for NPH is surgical and involves implanting a shunt system to divert excess CSF from the brain to another part of the body where it can be absorbed.
VP Shunt Surgery (Ventriculoperitoneal Shunt)
A VP shunt is the most commonly used surgical option for NPH. In this procedure, a thin tube (catheter) is inserted into the enlarged ventricles of the brain. The tube is tunnelled under the skin and connected to the abdominal cavity (peritoneum), where the CSF drains and is absorbed naturally by the body.
Modern shunt systems use programmable valves, which allow the neurosurgeon to noninvasively adjust the valve’s pressure setting after surgery using an external programmer. This fine-tuning is critical because different patients need different drainage pressures, and the ability to adjust without re-operation significantly improves outcomes and reduces revision surgery rates.
A seven-year retrospective study of NPH patients treated with programmable shunt valves found that 87.5% experienced good-to-excellent symptom relief, demonstrating the effectiveness of modern shunt technology when applied to appropriate candidates.
Learn more: VP Shunt Surgery in Delhi
Endoscopic Third Ventriculostomy (ETV)
In select cases, ETV may be considered as an alternative to shunt surgery. This procedure creates a new opening in the floor of the third ventricle, allowing CSF to bypass the obstruction and flow normally. ETV is more commonly used for obstructive hydrocephalus but may have a role in certain NPH presentations.
The Takeaway
Normal Pressure Hydrocephalus doesn’t get talked about enough, and that silence costs people years of quality life. The shuffling walk, the mental fog, the bathroom urgency, these aren’t just “getting old.” For many patients, these symptoms are fixable.
The frustrating part is that NPH looks so much like conditions that can’t be reversed. That’s exactly why the right diagnosis matters. A VP shunt won’t help an Alzheimer’s patient, but for someone with NPH, it can mean walking unassisted again, thinking more clearly, and reclaiming independence they thought was gone for good.
If something feels off and the pieces seem to fit, trust that instinct. An early conversation with a neurosurgeon costs far less than years of mismanaged decline.
