Revision Spine Surgery with Nerve Decompression

Reach Out for Expert Care
Four Surgeries. Years of Pain. She Finally Got Her Life Back.
At a Glance
| Patient | 53-year-old female |
| Complaint | Severe lower back pain; shooting pain down the right leg |
| Background | Three prior spine surgeries elsewhere; symptoms persisted and worsened |
| Procedure | Re-exploration of previous surgical site; right foraminotomy; removal of retained implant |
| Outcome | Significant pain relief; right leg symptoms resolved |
A 53-year-old woman came to Dr. Vikas Gupta carrying years of pain and years of disappointment. She had already been through multiple spine surgeries. Each time, she had hoped it would be the last. Each time, the pain had come back.
By the time she arrived, the pain in her lower back was severe, and a sharp, shooting pain was running down her right leg, making it difficult to sit, stand, or move without discomfort. She had been living like this for a long time.
This was her fifth surgery. And this time, it had to work.

Pre-operative X-ray : X-ray showing the previously operated spine with retained implant at L4-L5.
What does the scans show?
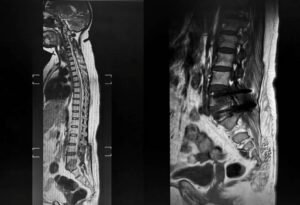
Pre-operative MRI: MRI showing the L4-L5 level with scar tissue formation and nerve compression on the right side.
The MRI told a familiar but complicated story. The L4-L5 level of her spine, the same level that had been operated on before, was showing significant scarring from the previous surgeries. The nerve root on the right side was being compressed, which explained the shooting pain travelling down her right leg. This is called radiculopathy, when a nerve in the spine is pinched or irritated, it sends pain, numbness, or weakness along the path that nerve travels.
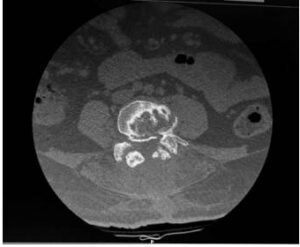
Pre-operative CT Scan: CT scan showing retained implant at L4-L5 and the extent of bony changes from previous surgeries.
The CT scan revealed something important: a retained implant from a previous surgery was still present at the L4-L5 level, and it was contributing to the problem. The bony anatomy around the previous surgical site had changed significantly, and the exit point of the nerve on the right side had narrowed, adding to the compression.
The Challenge
Revision spine surgery, going back into a spine that has already been operated on, is significantly more complex than a first-time procedure. Each previous surgery leaves behind scar tissue, altered anatomy, and changed bone structure. The surgical landmarks that a spine surgeon normally relies on are no longer where they should be.
For this patient, the challenge was threefold. First, navigating through dense scar tissue from three prior surgeries to safely reach the problem area. Second, identifying and removing the retained implant without damaging the surrounding nerves. Third, performing a foraminotomy, widening the narrowed exit point of the compressed nerve, in a spine that had already been significantly altered by previous operations.
This is the kind of surgery that requires not just technical skill, but deep familiarity with complex, previously operated spines.
Procedure: What Was Done?
Dr. Vikas Gupta performed a careful re-exploration of the previous surgical site at L4-L5.
Working through the scar tissue from prior operations, the retained implant was identified and safely removed. With the implant out, attention turned to the compressed nerve on the right side.
A right foraminotomy was then performed, a procedure in which the bony opening through which the nerve exits the spine is carefully widened. Think of it as opening a narrowed doorway so the nerve has enough space to pass through without being pinched. This directly addressed the shooting pain travelling down her right leg.
The problematic retained implant had been removed, and new implants were placed at L4-L5 providing the correct and stable fixation that the previous surgery had failed to achieve. The spine was now properly supported at the right level.
The surgery was completed without complication.

Post-operative X-ray: Post-operative X-ray confirming implant removal and the re-explored L4-L5 level.
Outcome
Following surgery, the patient experienced significant relief from her lower back pain, and the shooting pain down her right leg, which had been one of her most debilitating symptoms, resolved after the procedure.
For a woman who had spent years going through surgeries and still waking up in pain, this outcome was not a small thing. It was the relief she had been looking for through three previous attempts.
Why does this case matter?
Failed or incomplete spine surgery is more common than many people realise, and it is one of the most difficult situations a patient can find themselves in. The pain continues. The trust in the process erodes. And the decision to go through another surgery feels enormous.
What this case shows is that persistent pain after spine surgery is not something that simply has to be accepted. In many cases, there is a clear, identifiable reason why the previous surgery did not provide relief, whether it is a retained implant, a compressed nerve that was not adequately addressed, or scar tissue causing new problems. When that reason is found and treated correctly, meaningful recovery is still possible.
The right diagnosis matters as much as the right surgery. A thorough evaluation, with updated MRI, CT, and X-ray, is the essential first step before any revision procedure is considered.
If you or someone you know is still living with pain after spine surgery, it is worth seeking a specialist opinion. A second opinion is not a sign of giving up on your previous treatment, it is a step toward finding what was missed.
Still in pain after a spine surgery? Book a consultation for a thorough evaluation and an honest second opinion.
This case study is published for educational and awareness purposes only. It does not constitute medical advice.
