Slip Disc vs Sciatica: How to Tell the Difference

When your back starts hurting, or a sharp pain shoots down your leg, it is easy to assume the worst or, perhaps more commonly, to assume you already know what is wrong.
“It must be my slip disc.” “I think I have sciatica.” These two terms are used so frequently, and often interchangeably, that many people arrive at a clinic already convinced of their own diagnosis.
Here is what is important to understand: slip disc and sciatica are not the same condition. One can cause the other, but they are distinct problems that sometimes require different treatment approaches. Getting the distinction right is the first step toward getting better.
Reach Out for Expert Care
What Is a Slip Disc?
The spine is made up of a series of bones called vertebrae, cushioned between them by soft, gel-filled structures called intervertebral discs. These discs act as shock absorbers, allowing the spine to bend, twist, and carry load without bone grinding against bone.
A slip disc, medically known as a herniated or prolapsed disc, occurs when the soft inner material of a disc pushes outward through a weakened or torn outer layer. This can happen gradually over years of wear, or suddenly after a sharp movement or heavy lift.
The disc itself does not literally slip out of place. What happens is a bulge or rupture that can press against nearby structures, including the spinal cord or the nerve roots that branch out from it.
This pressure is what causes the symptoms.
What Is Sciatica?
Sciatica is not a diagnosis in itself. It is a symptom, specifically the pain, tingling, numbness, or weakness that travels along the path of the sciatic nerve.
The sciatic nerve is the longest nerve in the human body. It originates in the lower back, passes through the buttocks, and runs down the back of each leg all the way to the foot. When this nerve or any of the roots that form it becomes compressed or irritated, pain can radiate along its entire length.
Most people with sciatica describe a burning or electric shock-like sensation that travels from the lower back or buttock down through the leg, sometimes reaching the calf or foot.
Sciatica is a consequence. Something is pressing on or irritating the sciatic nerve. The real question is always: what is causing that irritation?
So, What Is the Relationship Between the Two?
A slip disc is one of the most common causes of sciatica.
When a herniated disc in the lumbar spine bulges outward, it can press directly onto one of the nerve roots that form the sciatic nerve. This pressure then causes the classic shooting pain down the leg that most people associate with sciatica.
However, sciatica can also be caused by other conditions, including:
- Spinal canal narrowing (lumbar stenosis)
- A slipped vertebra pressing on a nerve (spondylolisthesis)
- Piriformis syndrome, where a muscle in the buttocks compresses the nerve
- Tumours or cysts near the spinal canal, though these are rarer
This is why assuming you have a slip disc just because you have leg pain, or assuming you have sciatica just because your back hurts, can lead to confusion and delayed treatment.
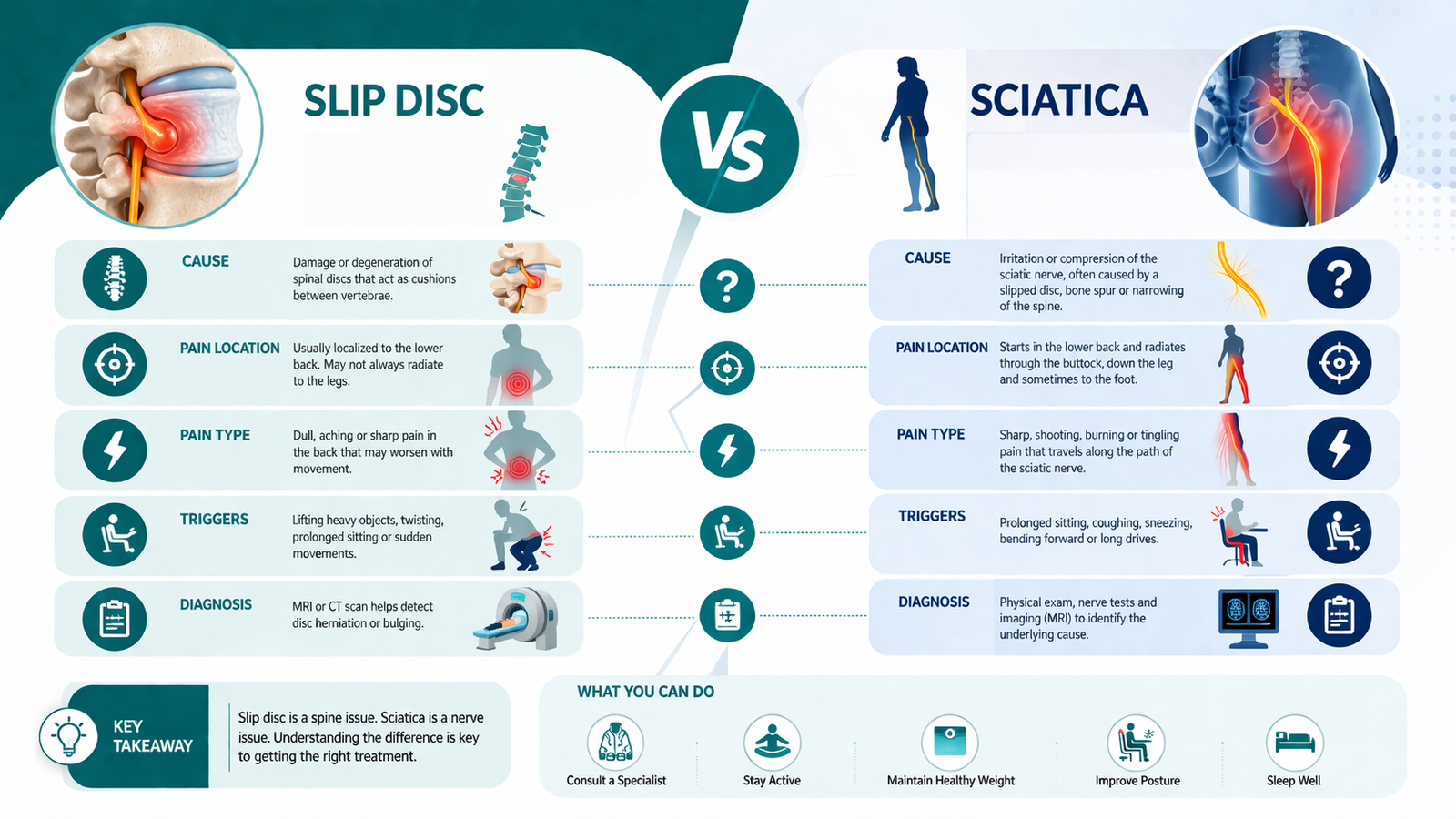
Slip Disc vs Sciatica: How the Symptoms Differ
Understanding where the pain is, how it feels, and what makes it better or worse can offer useful clues.
Slip Disc Symptoms
A slip disc does not always cause leg pain. In some cases, it causes primarily back pain, stiffness, or localised tenderness. The pain may worsen when bending forward, sitting for long periods, or straining.
If the herniated disc is pressing on a nerve, symptoms may include:
- Sharp or burning pain radiating into the buttock or leg
- Numbness or tingling in the leg or foot
- Muscle weakness in the affected leg
- Pain that worsens with coughing, sneezing, or prolonged sitting
Sciatica Symptoms
Sciatica almost always involves leg pain, and this is its defining feature. The pain typically follows the course of the sciatic nerve, running from the lower back or buttock down through the thigh, calf, and sometimes into the foot.
People commonly describe it as:
- A sharp, shooting, or electric sensation down one leg
- A deep ache or burning feeling in the buttock or thigh
- Numbness, pins and needles, or weakness below the knee
- Pain that is often worse when sitting, standing for too long, or getting up from a chair
The key distinction is this: back pain alone is more suggestive of a disc problem. Leg pain following a specific nerve path is the hallmark of sciatica. When both occur together, a herniated disc compressing a nerve root is often the explanation.
“But Doctor, My Pain Is Everywhere. How Can Anyone Tell?”
This is a question Dr. Vikas Gupta hears often.
“Patients frequently arrive having self-diagnosed using information they found online, sometimes correctly, but often partially. The challenge is that these conditions overlap significantly in their presentation. A thorough clinical examination, combined with the right imaging, is what separates assumption from accurate diagnosis.”
A neurological examination looks at reflexes, muscle strength, and sensation in the legs. Specific tests, such as the straight leg raise, can help identify nerve root irritation. Imaging, particularly an MRI of the lumbar spine, provides a detailed picture of disc health, nerve compression, and the condition of surrounding structures.
One patient described their experience: “I had been managing my back pain for months, assuming it was just a muscle strain. When the shooting pain started going into my leg, I finally came to see Dr. Vikas Gupta. An MRI showed a herniated disc pressing on a nerve. Once I understood what was actually happening, the treatment made so much more sense.”
When Should You Seek Medical Attention?
Many episodes of back pain and mild sciatica improve with rest, physiotherapy, and anti-inflammatory medication over several weeks. However, certain symptoms should prompt medical evaluation:
- Pain that is severe or getting progressively worse
- Weakness in the leg, particularly difficulty lifting the foot
- Numbness or tingling that is spreading or worsening
- Loss of bladder or bowel control, which requires urgent assessment
- Symptoms persisting beyond six to eight weeks without improvement
Dr. Vikas Gupta advises, “Do not wait until you cannot walk properly to seek help. Early diagnosis means more options and a faster, more complete recovery. Some patients who delay end up with nerve damage that takes far longer to heal, or in some cases may not fully resolve.”
Treatment: Does It Differ for Slip Disc and Sciatica?
Because sciatica is often caused by a slip disc, the treatment frequently overlaps. However, the approach depends on the underlying cause identified through diagnosis.
Conservative Management (First-Line for Most Cases)
- Physiotherapy focused on core strengthening, posture correction, and nerve mobilisation
- Pain relief through anti-inflammatory medications
- Hot or cold therapy for symptomatic relief
- Gradual return to activity, avoiding prolonged bed rest
Interventional Options
- Nerve root injections or epidural steroid injections to reduce inflammation around a compressed nerve
- These are typically considered when conservative treatment has not provided adequate relief
Surgical Treatment
Surgery is reserved for cases where nerve compression is severe, neurological deficits are progressing, or conservative treatment has failed after an appropriate period. A microdiscectomy, where the portion of disc pressing on the nerve is carefully removed, is the most common procedure for disc-related sciatica.
“Surgery is not the first conversation I have with most patients,” Dr. Vikas Gupta explains. “The majority of people with a slip disc or sciatica get better with the right conservative care. Surgery becomes the right choice when the nerve is under significant ongoing pressure, or when the quality of life is so severely impacted that waiting longer causes more harm than good.”
Another patient shared: “I was terrified I would need surgery when the pain in my leg became unbearable. Dr. Vikas Gupta assessed me thoroughly and recommended a nerve root injection followed by physiotherapy. Within a few weeks, the pain had reduced dramatically. I avoided surgery and I am back to my normal routine.”
Looking After Your Spine Before Problems Begin
For many people, slip discs and sciatica are not inevitable. The health of the spine is significantly influenced by daily habits.
Protective measures include:
- Maintaining a healthy weight to reduce load on lumbar discs
- Strengthening the core muscles that support the spine
- Practising good posture, especially during prolonged sitting
- Lifting correctly by bending the knees rather than the back
- Staying physically active rather than leading a sedentary lifestyle
- Addressing ergonomics at work, particularly for desk-based roles
Dr. Vikas Gupta adds, “The spine is remarkably resilient, but it responds to how we treat it over decades. Small, consistent choices about posture, movement, and exercise have a cumulative protective effect that no treatment can fully replicate after the fact.”
The Right Diagnosis Makes All the Difference
Slip disc and sciatica are terms that are often confused, conflated, and self-diagnosed. While one frequently causes the other, they are distinct conditions that deserve accurate evaluation.
If you have been living with back pain, leg pain, or a combination of both, and are uncertain what is actually causing it, a proper neurological assessment and appropriate imaging can provide clarity.
Understanding your diagnosis is not just reassuring. It is the foundation of effective treatment.
